It Begins With You
Motivation and Readiness -> FrameworksAlmost all of the approaches to assess motivation and readiness to change are based on two models: the Transtheoretical Model and motivational interviewing. The following are described below:
- The Transtheoretical Model, including Stages of Change and the Processes Supporting that Change and University of Rhode Island Change Assessment Scale (URICA)
- Motivational Interviewing
The Transtheoretical Model
The Transtheoretical Model is an integrative, biopsychosocial model that can be applied to a variety of behaviors, which is why it is called “trans-theoretical.” As shown in the diagram below, there are five stages of change: precontemplation, contemplation, preparation, action and maintenance.(Drawn from Prochaska & DiClemente, 1983; Prochaska, DiClemente, & Norcross, 1992)
 Source: https://www.prochange.com/transtheoretical-model-of-behavior-change
Source: https://www.prochange.com/transtheoretical-model-of-behavior-change
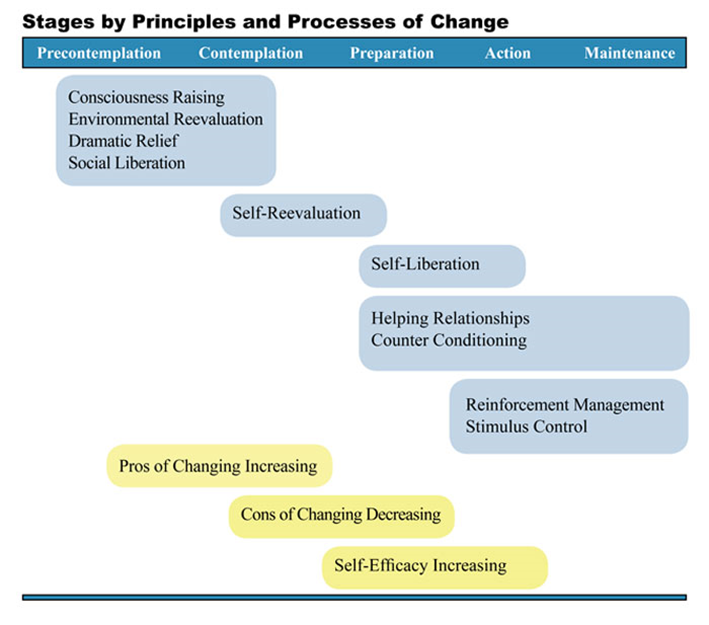
Stages of Change and the Processes Supporting that Change
Certain common change processes take place to move someone from one stage of change to the next. Each stage along with common processes are described below and in the next diagram.
Precontemplation stage: People in this stage do not plan to take action in the near future, and may be uninformed about the consequences of their action. Change processes include:
- Consciousness raising – awareness about the causes and consequences of their behavior
- Dramatic relief – recognizing the relief that will come with behavior change
- Environmental evaluation – noticing one’s effect on others
- Social liberation – more public support for people engaging in healthy behaviors
Contemplation stage: In this stage, people plan to make a change in the next six months. They are ambivalent about change as they know the pros of changing, but are also aware of the cons. The main change process is:
- Self-Reevaluation – realizing that healthy behavior change is an important part of one’s identity.
Preparation stage: During preparation, individuals intend to take action within the next month by joining a health education class, consulting a counselor, talking to a physician, or buying a self-help book. The change processes are:
- Self-liberation – making the commitment to make the change and believing in one’s capability to do so.
- Helping Relationships – seeking and using social support such as peer groups, mentors or counselors, to make and sustain changes.
- Counter Conditioning – Substituting healthy behaviors for problem behaviors, such as walking as a substitute for comfort foods as a way to cope with stress.
Source: https://www.prochange.com/transtheoretical-model-of-behavior-change
Action stage: This is the stage in which individuals have made healthy changes to their behaviors within the past six months.
- Reinforcement Management – Seeing the rewards of change, and reinforcing themselves through self-talk such as, “Nice going – you handled that temptation.”
- Stimulus Control – Removing triggers for unhealthy habits, such as removing all the ashtrays from the house and car for someone who is quitting smoking.
Maintenance stage: In this stage people are working to prevent relapse. They are less tempted to relapse and become more confident that they can keep their changes in place.
As an individual moves toward action, the pros of changing increase, the cons decrease, and self-efficacy increases, meaning one believes that one is capable of sustaining change.
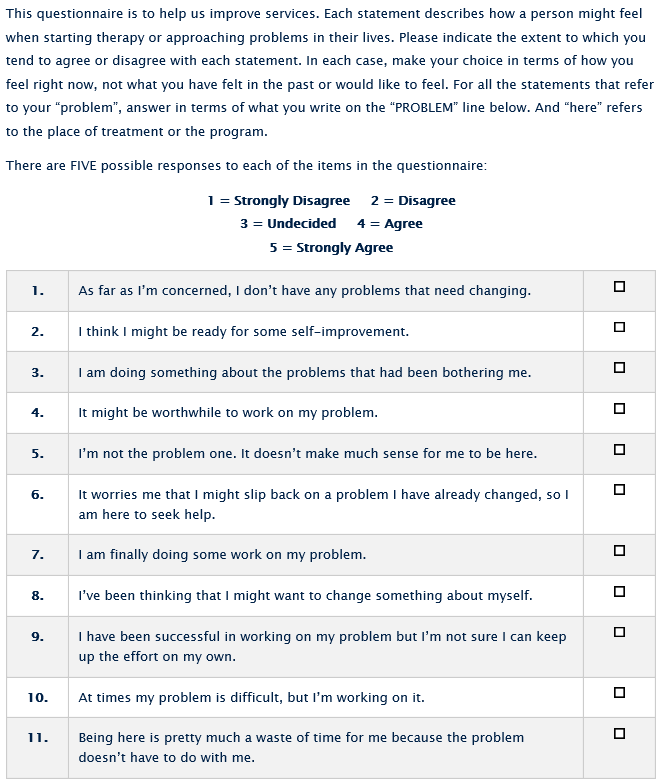
University of Rhode Island Change Assessment Scale (URICA)
The University of Rhode Island Change Assessment Scale is a 32-item self-report tool that can help someone see in what stage(s) of change he or she resides. The tool was developed by one of the founders of the model, Dr. James Prochaska, who is now professor of psychology and director of the Cancer Prevention Resource Center at the University of Rhode Island where he has continued his work on the Transtheoretical Model in that role. Sample questions from the tool are shown below. A scoring legend indicates which questions are associated with which stage of change. The scale is designed to be a continuous measure so subjects can score high in more than one of the four stages.
University of Rhode Island Change Assessment – Excerpt
Source: University of Rhode Island’s Cancer Prevention Research Center
Motivational Interviewing
Motivational interviewing (MI) is a therapeutic style that was first used with problem drinkers. The fundamental concepts were later described in a psychotherapy journal in 1983. The founders of the model, William R. Miller and Stephen Rollnick, wrote a book in 1991 that further described the model as one in which the goal was for the helper to persuade rather than coerce, and to be supportive rather than argumentative.
Motivational interviewing is a conversational approach designed to help people (See Case Western Reserve University’s Center for Evidence-Based Practices):
- Discover their own interest in considering and/or making a change in their life (e.g., diet, exercise, managing symptoms of physical or mental illness, reducing and eliminating the use of alcohol, tobacco, and other drugs)
- Express in their own words their desire for change (i.e., “change-talk”)
- Examine their ambivalence about the change
- Plan for and begin the process of change
- Elicit and strengthen change-talk
- Enhance their confidence in taking action and noticing that even small, incremental changes are important
- Strengthen their commitment to change
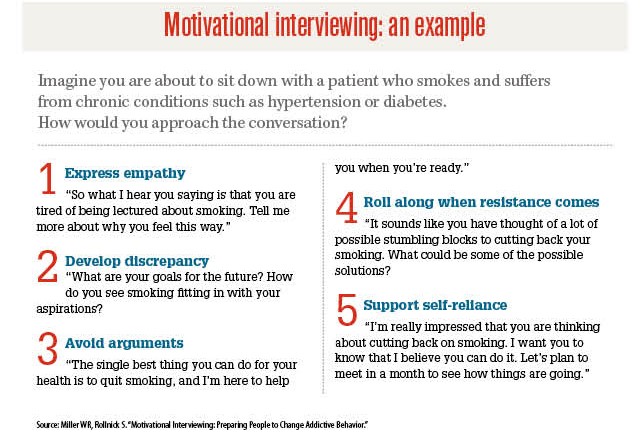
The clinician needs to have a strong sense of purpose and have the skills and good timing to intervene at the most opportune moments, while keeping the five following principles in mind (SeeMiller and Rollnick, 1991, pp. 51-52):
- Express empathy through reflective listening.
- Identify the discrepancy between the clients’ goals or values and their current behavior.
- Avoid argument and direct confrontation.
- Adjust to client resistance rather than opposing it directly.
- Support self-efficacy and optimism.
The following diagram gives good examples of what the clinician might say for each of these principles.
 MI is one of the core components of a variety of interventions used by direct-service providers, supervisors, team leaders, and organizations in the following service areas (See Case Western Reserve University’s Center for Evidence-Based Practices):
MI is one of the core components of a variety of interventions used by direct-service providers, supervisors, team leaders, and organizations in the following service areas (See Case Western Reserve University’s Center for Evidence-Based Practices):
- Substance abuse (addiction services)
- Mental health
- Psychiatry
- Primary healthcare
- Nursing
- Supported employment
- Tobacco cessation & recovery
- Vocational rehabilitation
- Residential
- Housing
- Healthcare
- Criminal justice